
Iron is required for all living cells and a deficiency of this element significantly impacts cellular function, regardless of whether the cells are erythroid progenitors, neurons or cardiomyocytes. Thus, all physicians caring for infants and toddlers should be knowledgeable about optimal means of preventing iron deficiency (ID) by using effective feeding strategies in normal and very low birth weight (VLBW) neonates, as well as later in infancy when iron requirements remain high due to continued rapid growth.21
Daily Iron Requirements for Infants and Young Children
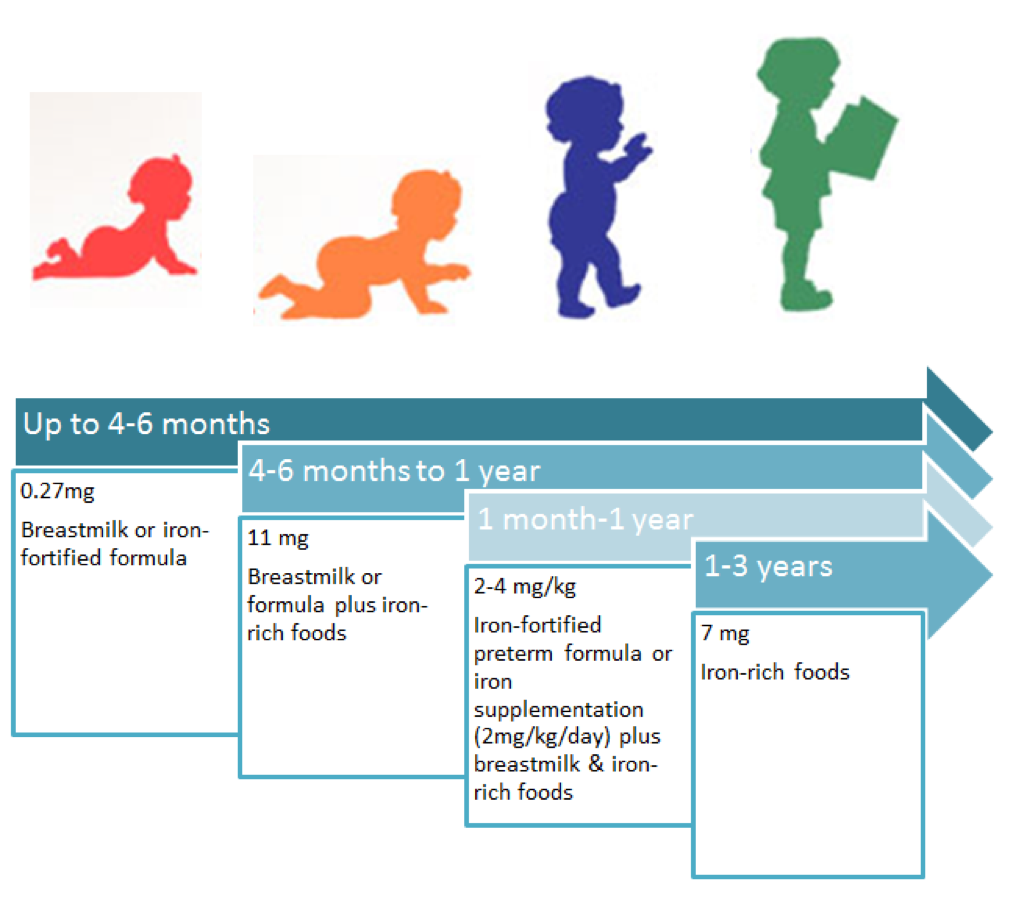 *The majority of a newborn’s iron is acquired during the third trimester. Therefore, premature infants require more iron than term infants due to poor fetal iron endowment.
*The majority of a newborn’s iron is acquired during the third trimester. Therefore, premature infants require more iron than term infants due to poor fetal iron endowment.
Figure adapted from: Janus J, Moerschel SK. Evaluation of Anemia in Children. Am Fam Physician 2010;81(12)1462-71. And https://www.emaze.com/@ALLQTWFZ/infants-power-point-new-(1).pptx
Summary of Screening Recommendations
Screening
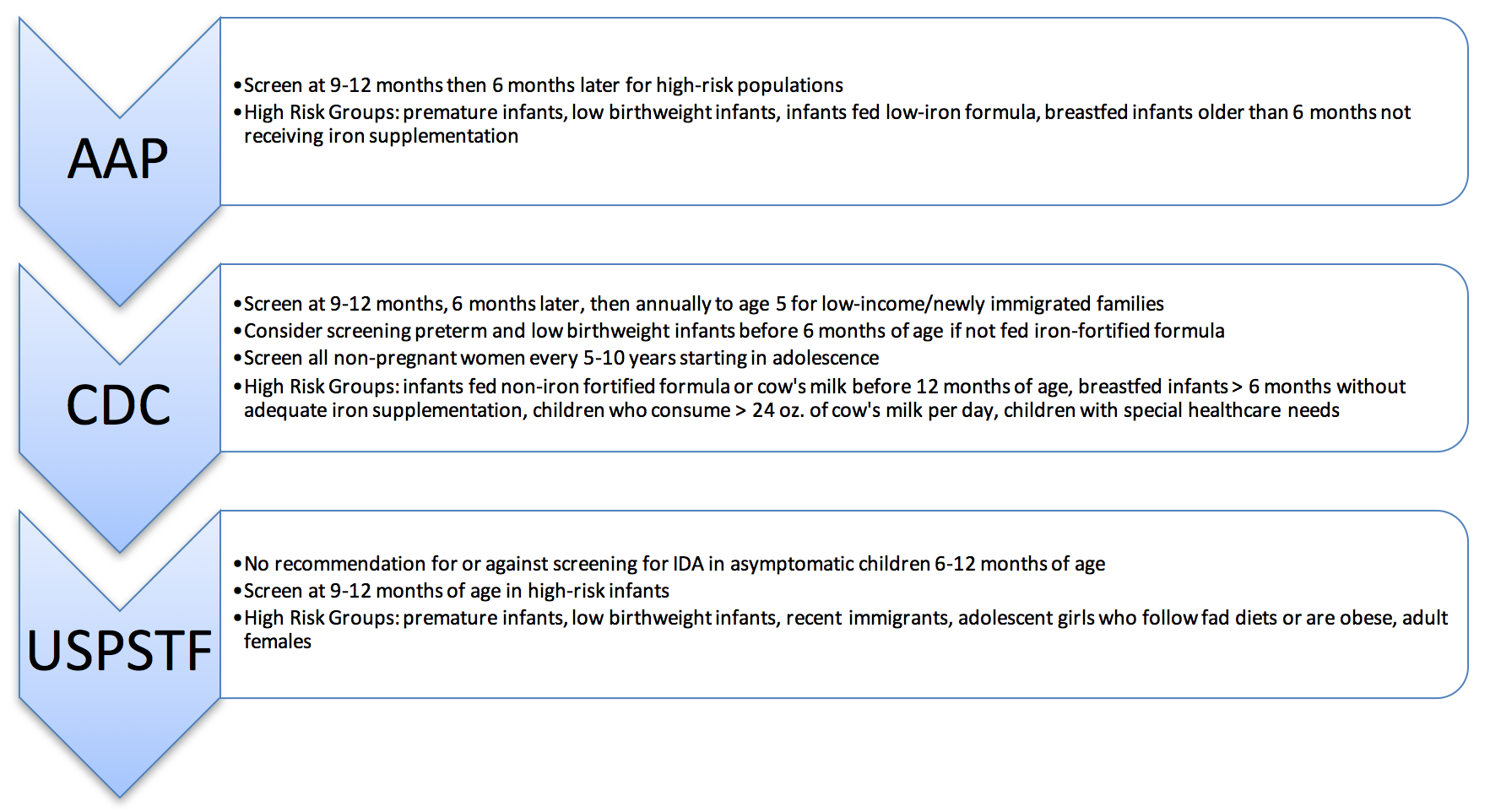
Comparison of Recommendations for Screening for Anemia
 Click figure for larger version.
Click figure for larger version.
Figure above adapted from: Janus J, Moerschel SK. Evaluation of Anemia in Children. Am Fam Physician 2010;81(12):1462-71. Additional Sources: 22, 23, 24.
When should I screen my patient?
- The AAP recommends screening all patients for IDA using Hb/Hct at 12 months of age.
- UW Clinics recommend universal screening for ID using CBC and ferritin at 12 months of age.
- Patients with ≥ 1 risk factor should be screened earlier since the sooner ID/IDA is treated, the less severe the consequences.
- What tests should I order?
- Iron stores are best determined through measures of serum ferritin level and can detect iron deficiency before it progresses to IDA.
- Anemia can be detected with a CBC.
Interpreting Results
Screening Questions
Prior to embarking on the empiric trial of iron supplementation, every child should have a careful dietary history and review of risk factors for lead exposure.25
Although screening questions provide useful information, they are not sufficient to identify all children with ID or IDA. These should be used as a supplementary screen, not a primary screen.
Laboratory Findings in the Differential Diagnosis of Iron Deficiency
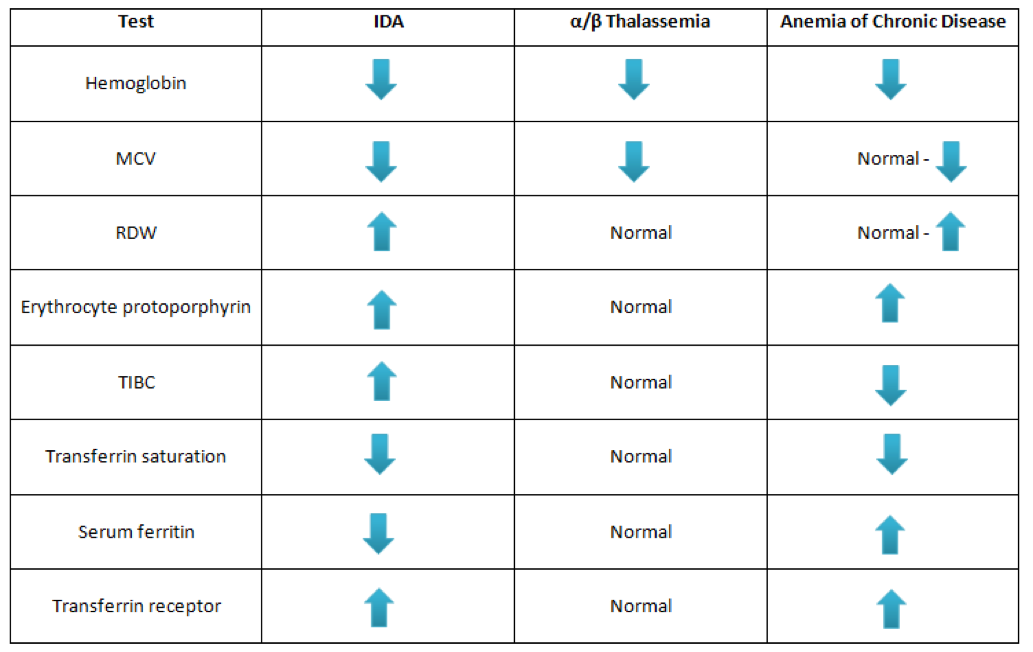
Table above adapted from: Mahoney DH. Iron deficiency in infants and young children: Treatment. In: UpToDate, Motil KJ, Drutz JE, Hoppin AG (Eds), UpToDate, Waltham, MA. (Accessed July 6, 2015).
Evaluation
Evaluation of Low Hemoglobin Levels
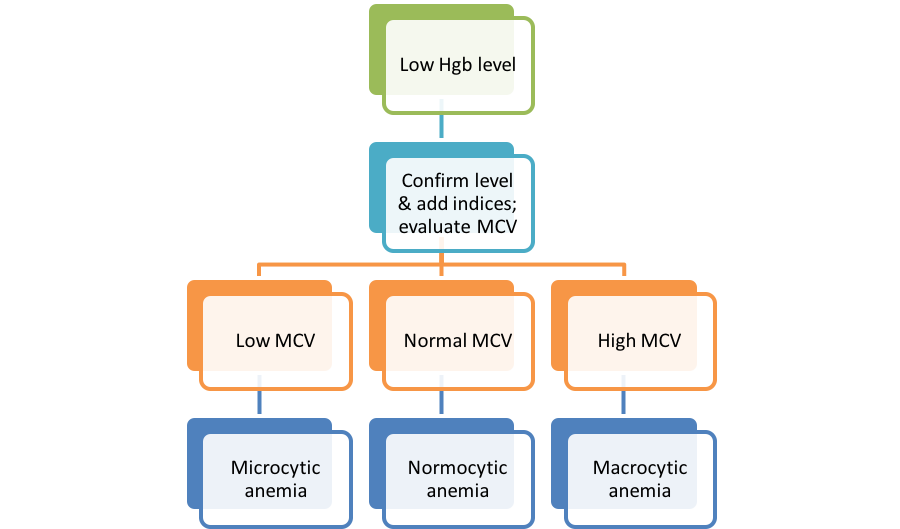
If an individual has microcytic anemia, the next question to ask is whether the anemia is mild and if the history and iron indices are consistent with ID/IDA.
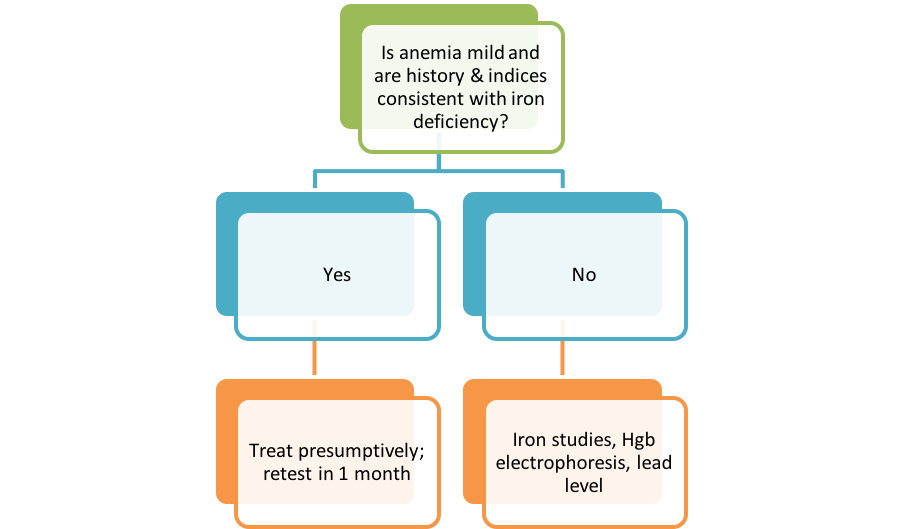
If the anemia is mild and the history/iron indices are consistent with ID/IDA, then treatment should begin. Iron indices should be retested in one month and if hemoglobin has increased by > 1.0 g/dL, then the diagnosis of iron deficiency is confirmed. As a result, you should counsel the family about cow’s milk consumption while continuing treatment for another 1-2 months.
If the anemia is not mild or the history/indices are inconsistent with iron deficiency, iron studies, hemoglobin electrophoresis and lead level tests should be performed. The possible outcomes of these tests are shown in the figure below.
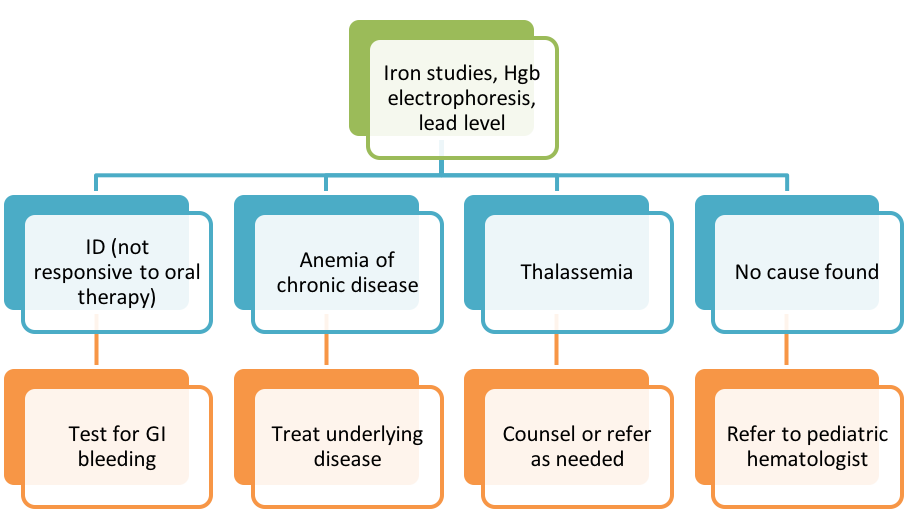
Figures above adapted from Janus J, Moerschel SK. Evaluation of Anemia in Children. Am Fam Physician 2010;81(12):1462-71.
Causes of IDA
Causes of Recurrent or Refractory Iron Deficiency Anemia (IDA) in Infants and Children
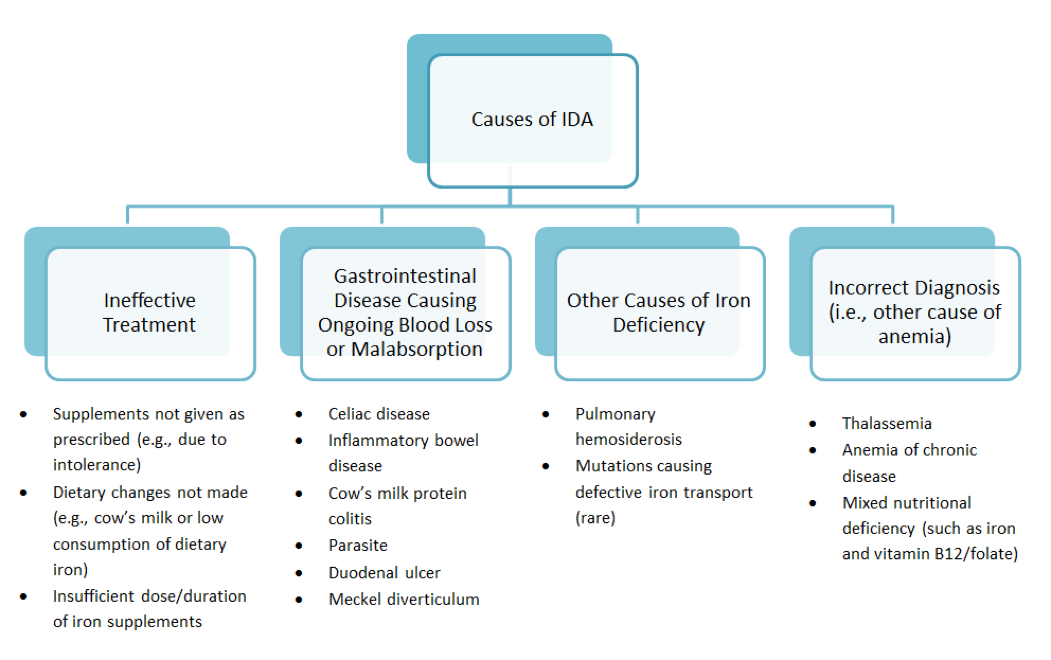
Figure adapted from: Mahoney DH. Iron deficiency in infants and young children: Treatment. In: UpToDate, Motil KJ, Drutz JE, Hoppin AG (Eds), UpToDate, Waltham, MA. (Accessed July 6, 2015)